

Click here to download this post
Dr. DePace, MD, FACC
Dr. Joseph Columbo
Note: This is an article recently published by Springer in their “Current Cardiology Reports” on their website. The Abstract is printed here. The entire article is availalbe by clicking this link or downloading it as a PDF
Abstract
Purpose of Review
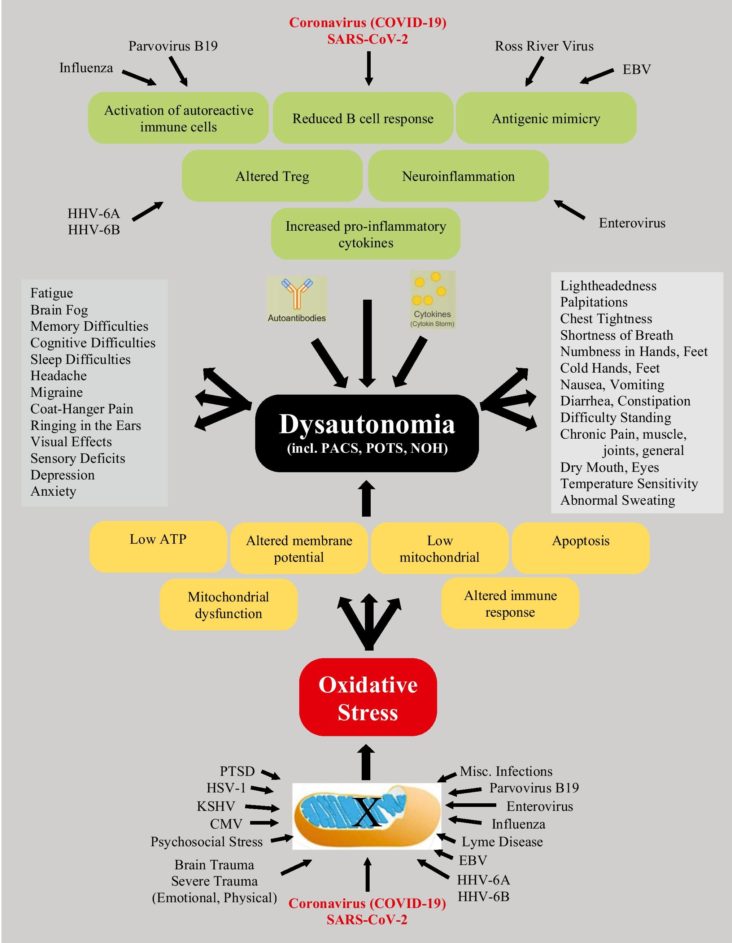
Long-COVID syndrome is a multi-organ disorder that persists beyond 12 weeks post-acute SARS-CoV-2 infection (COVID-19). Here, we provide a definition for this syndrome and discuss neuro-cardiology involvement due to the effects of (1) angiotensin-converting enzyme 2 receptors (the entry points for the virus), (2) inflammation, and (3) oxidative stress (the resultant effects of the virus).
Recent Findings
These effects may produce a spectrum of cardio-neuro effects (e.g., myocardial injury, primary arrhythmia, and cardiac symptoms due to autonomic dysfunction) which may affect all systems of the body. We discuss the symptoms and suggest therapies that target the underlying autonomic dysfunction to relieve the symptoms rather than merely treating symptoms. In addition to treating the autonomic dysfunction, the therapy also treats chronic inflammation and oxidative stress. Together with a full noninvasive cardiac workup, a full assessment of the autonomic nervous system, specifying parasympathetic and sympathetic (P&S) activity, both at rest and in response to challenges, is recommended. Cardiac symptoms must be treated directly. Cardiac treatment is often facilitated by treating the P&S dysfunction. Cardiac symptoms of dyspnea, chest pain, and palpitations, for example, need to be assessed objectively to differentiate cardiac from neural (autonomic) etiology.
Summary
Long-term myocardial injury commonly involves P&S dysfunction. P&S assessment usually connects symptoms of Long-COVID to the documented autonomic dysfunction(s).